

Basic human permanent dentition. Click to enlarge. Image credit: modified from here.
Teeth, as a part of the dentition, are a wonder of the natural world and come in a variety of forms and designs in vertebrate animals, with perhaps some of the most impressive examples include the tusks of elephants and walruses. They are also the only part of the human skeletal system that can be observed naturally and the only part that interact directly with their environment via mastication (White & Folkens 2005: 127).
Although primarily used to break down foodstuffs during mastication, teeth can also be used as tools for a variety of extramasticatory functions such as the processing of animal skins and cord production (Larsen 1997: 262). As the hardest of the biological material found in the body teeth survive particularly well in both the archaeological and fossil records, often surviving where bones do not. Teeth are a goldmine of information for the human osteologist and forensic anthropologist alike as they can be indicative of the sex, age, diet and geographic origin of the individual that they belong to (Koff 2004, Larsen 1997, Lewis 2009, White & Folkens 2005).
This entry will introduce the basic anatomy of the human dental arcade, deciduous and permanent dentition and the various tooth classes, alongside a quick discussion of the action of mastication itself. But first, as always in this series, we’ll take a look at how teeth can be found during the excavation of archaeological sites. This post marks the final Skeletal Series post to deal explicitly with individual elements of the human skeletal system. The next few posts in the Skeletal Series will be aimed at detailing the methods used in aging and sexing elements in the adult and non-adult skeleton (and the success rates of the various methods), followed by posts introducing the pathological conditions that can be present on human skeletal remains.
Excavation
The 32 permanent human teeth, located in the upper arcade (maxilla) and lower arcade (mandible) of the jaws, each holding 16 teeth, are resilient to chemical and physical degradation. Furthermore tooth crown morphology (the surface that consists of enamel) can only be changed by attrition (tooth wear), breakage, or demineralization once the crown of a tooth has erupted through the gum line (White & Folkens 2005: 127). As such teeth are often found at locations where human remains are suspected to be buried or otherwise excavated. Care must be taken around the fragile bones of the spanchnocranium (i.e. the facial area of the skull), defined as necessary, and, if needed due to fragility, the area may have to be lifted with natural material still adhered to the bone to be more carefully micro-excavated in the lab (Brothwell 1981: 3).

Circled in red, the teeth are located in the upper (maxilla) and lower (mandible) jaws. This individual, dating to the medieval period in eastern Germany, highlights a common occurrence in supine burials where the mandible often ‘falls’ forward as the muscles, ligaments and tendons decompose. Always be careful when excavating suspected burial features as both bone and tooth can be chipped by trowels or other metallic excavation implements. Photograph taken by author.
Loose dentition may be found around the skull itself as teeth can be loosened naturally postmortem as natural ligaments decompose. Sieving around the location of the skull may prove useful in finding loose teeth and also the smaller bones of the skulls (such as the ear ossicles). In the excavation of non-adult remains, or of suspected females with fetal remains in-situ, great care should be taken in recording and the excavating of the skull, torso and pelvis. As mentioned below teeth form from the crown down, as such deciduous or permanent teeth during growth may be loose in exposed crypts in the mandible or maxilla (Brickley & McKinley 2004). Furthermore due to the small size and colour of the 20 deciduous teeth, especially the crowns during the formation and growth of the teeth, may be mistaken for pieces of dirt or rocks.
Tooth Anatomy & Terminology
The basic anatomy of teeth can be found in the diagram below, but it is worth listing the anatomical features of a typical tooth here. The chewing surface of the tooth is called the occlusal surface and it is here that the crown of the tooth can be found. The crown of a tooth is made of enamel, an extremely hard and brittle mixture of minerals (around 95-96% hydroxyapatite). The enamel is formed in the gum and once fully formed contains little organic material. The demineralization of teeth can repair initial damage, however this is limited in nature. Dentin (sometimes termed dentine) is the tissue that forms the core of the tooth itself. It is supported by a vascular system in the pulp of the tooth. Dentin can only repair itself on the inner surface (the walls of the pulp cavity), but dentin is a softer material than enamel and once exposed by occlusal wear it erodes faster than enamel. The pulp chamber, in the centre of the diagram below, is the largest part of the pulp cavity at the crown end of the tooth. The pulp itself is the soft tissue inside the pulp chamber, which includes the usual trio bundle of vein, artery and nerves (V.A.N.). The root of the tooth is the part that anchors it into the dental alveolus tissue (sockets) of the jaw (either the maxilla or mandible).

The basic anatomy of a tooth (in this case a molar), outlining the three main layers present in all human teeth. Image credit: Kidport.
Cementum is the bone type tissue that covers the external surface of the roots of teeth. The apex, or apical foramen, is the opening at the end of each root, which allows for the nerve fibers and vessels up the root canal into the pulp chamber. Heading back up to the occlusal surface of the tooth we encounter cusps of the crown, each of which have different individual names depending on their position. Upper teeth end with the prefix -cone whereas lower teeth end with the prefix -conid (see details here). Finally we have fissures, which are clefts between the occlusal surfaces between cusps. Fissures help divide the cusps into patterns and are helpful to know to help identity individual teeth (specifically the molars). Above information taken from White & Folkens (2005: 130-131).
As previously highlighted there are some directional terms that are specific to the dentition, but it is pertinent to repeat some of the key aspects here for clarification as tooth orientation is important –
Apical: towards the root.
Buccal: towards the cheek (the buccinator muscle- the terminator of the muscle world!), used in realtion to posterior teeth (premolars and molars) only.
Cervical: towards the base of the crown or neck of the tooth (often called the cementoenamel junction).
Distal (direction): away from the midline of the mouth, opposite of mesial.
Incisal: towards the cutting edge of the anterior teeth.
Interproximal: between adjacent teeth, also useful to know and be able to identify are interproximal contact facets (IPCFs) which can indicate anatomical location of tooth.
Labial: surface towards the lips, anterior teeth (canines and incisors) only.
Lingual: of the tooth crown towards the tongue.
Mesial (direction): towards the midline, closest to the point where the central incisors contact each other.
Occlusal: towards the chewing surface (crown) of the tooth.

Tooth anatomical direction terminology and legend of tooth position, above is the maxillary dental arcade. Typically the uppercase and lowercase numbers refer to maxilla and mandible positions respectively, and often include a L or R for left or right hand side for quadrant location. In deciduous dentition lower case letters are used, in permanent dentition capitalization is used. Premolars are often 3rd (1st premolar) and 4th (2nd premolar) after palaeontological standards. Check out Brickley & McKinley (2004) below for BABAO recording standards. Image credit: Dr Lorraine Heidecker @ Redwoods.edu.
Above information taken from White & Folkens (2005: 128) and here.
A different method for recording the presence/absence and state of the individual teeth from archaeological skeletal populations is proposed by the British Association of Biological Anthropology and Osteoarchaeology (BABAO) as mentioned above. In this method, proposed by Connell (2004: 8) the deciduous and permanent dentition are given a separate letter or number:

The BABAO 2004 guidelines for compiling a dental inventory for a skeleton. It should be noted that if compiling a large inventory for a population it is best to individually number and identify each tooth after the Buikstra & Ubelaker 1994 standards (but see also Bone Broke). Click to enlarge. Image credit: Connell (2004: 8).
Deciduous & Permanent Teeth
Humans have only two sets of teeth during their lifetimes. The first set, known as the deciduous (primary or milk) teeth, are the first to form, erupt and function during the early years of life (White & Folkens 2005: 128). The primary dentition consists of central incisor, lateral incisor, canine, first molar and second molar in each jaw quadrant, making a total of 20 individual deciduous teeth in all.
These are systematically lost and replaced by the permanent, or secondary, dentition throughout childhood, adolescence and early adulthood. As noted above these include a central incisor, lateral incisor, canine, two premolars, and three molars in each jaw quadrant making a total of 32 individual permanent teeth in all.
The sequencing of the pattern of tooth eruption plays a vital clue in estimating the age of the individual, whilst tooth attrition (wear) is used in estimating individual age after the permanent dentition have fully erupted (White & Folkens 2005: 346). The loss of a tooth, or teeth, antemortem (before death) can lead to alveolar resorption over the empty tooth socket. Individuals who have no teeth left (often elderly individuals or individuals suffering periodontal disease) are termed edentulous. This can lead to problems pronouncing words, the cheeks sagging inwards and problems chewing or grinding food (Mays 1999). Perhaps the most famous example of this is one of the Dmanisi hominin fossils (crania D3444 and associated mandible D3900) whose crania lacked any teeth whatsoever and showed alveolar bone resorption of both the mandibular and maxillary arches. However, if this is evidence of conspecific care, or just of survival, is not known (Hawks 2005).

The human deciduous dentition, notice the absence of any premolars and lack of third molar. The total number of deciduous teeth is 20. Not to scale. Image credit: identalhub.
Deciduous tooth formation begins only 14-16 weeks after conception. White & Folkens (2005: 364) note that there are four distinct periods of emergence of the human dentition: 1) most deciduous teeth emerge and erupt during the 2nd/3rd year of life, 2) the two permanent incisors and first permanent molar usually emerge around 6-8 years old, 3) most permanent canines, premolars, and second molars emerges between 10-12 years old and finally 4) the 3rd molar emerges around 17/18 years old – although this can vary. Note also that there are some differences between the sexes and between populations (Larsen 1997, Lewis 2009, Mays 1999). Trauma, pathological conditions and diseases can also influence tooth development and eruption rates, often delaying the eruption of the permanent dentition and sometimes leaving visible deformities in the teeth themselves, such as linear enamel hypoplasia (sign of stress) or mulberry molars (specific sign of disease) (Lewis 2009: 41).

The human permanent dentition highlighting the 32 individual present. Notice the crown shape and sizes indicating different functions. Not to scale. Image credit: identalhub.
The basic differences between the deciduous and permanent dentition are as follows:
Deciduous…………………….Permanent
1. No premolars. 2 premolars.
2. Smaller teeth, each Larger teeth apart from premolars
tooth is smaller than which replace deciduous molars.
successor.
3. Cusps pointed & Cusps are blunt, crowns not bulbous,
crowns bulbous. contact areas broader.
4. Enamel less translucent, Enamel is more translucent, blueish white.
teeth appear whiter.
5. Enamel ends abruptly at Enamel ends gradually,
the neck. 1st molars have no bulge at cervical margin.
6. Occlusally the Bucco- Buccal and lingual surfaces do not converge,
lingual diameter therefore wider.
of molars is narrower.
7. Roots shorter and more Roots longer and stronger, multi-rooted
delicate, separate close teeth trunk present and roots
to crown, but are longer do not diverge near crown.
compared to crown size.
8. Dentin is less thick. Dentin is thicker.
9. Enamel more permeable Enamel less permeable, more calcified,
less calcified, more relatively less attrition.
attrition.
Above information modified from White & Folkens 2005 and here.
Tooth Class
Teeth in humans are classed into 4 separate classes of tooth based on function and position. The classes include incisors, canines, premolars and molars, each aiding the other during the mastication of food.

The human permanent dentition. Notice the larger size of the maxilla (upper) crowns compared to the mandible (lower) crowns and the differences between the roots of the same class of tooth. The first molar is the largest of the molar and the first to erupt. This can tooth can often have evidence of attrition on its cusps and crown when the 2nd and 3rd molars lack abrasion due to the 1st’s early eruption. Not to scale. Image credit: Biologycs 2012.
Maxilla Teeth:
Incisors (general: crowns flat and blade-like, outline of dentine occlusal patch is often rectangular or square if exposed by wear)
The upper incisor crowns are broad (or mesiodistally elongated) relative to their height, and have more lingual relief. The central incisor crown is larger and more symmetrical than the lateral incisor crown but the roots are shorter and stouter to crown size than to the lateral incisor roots (White & Folkens 2005: 142).
Canines (general: crowns are conical and tusklike, canine roots longer than other roots in the same dentition, can be confused for incisors)
Upper canines are broad relative to their height and have more lingual relief, with apical occlusal wear that is largely lingual (towards the tongue) (White & Folkens 2005: 139).
Premolars (general: crowns are round, shorter than canine crowns and smaller than molar crowns, generally only have two cusps, usually single rooted but can be confused for canines but note shorter crown height)
The upper premolar crowns have cusps of nearly equal size and the crowns are more oval in occlusal outline. Further to this the crowns of upper premolars also have strong occlusal grooves that orient mesiodistally between the major cusps, this is a key identifier for maxilla premolars (White & Folkens 2005: 140).
Molars (general: crowns larger, squarer, bear more cusps than any other tooth class, have multiple roots, 3rd molars sometimes mistaken for premolars)
Generally peaking the maxilla molars go from largest to smallest (1st molar to 3rd molar) in size and morphology. The crowns generally have 4 cusps. The 1st molar has three roots (two buccal and one lingual, which when seen from the buccal position the lingual root comes into view in the middle of the two buccal roots). The occlusal surface is described as a rhomboid in shape with 4 distinctive cusps. The 2nd molar has three roots but the two buccal roots are nearly parallel with each other, and is described as heart shape in the occlusal view. The 3rd molar has three roots present but the two buccal roots are often fused, and the outline of the occlusal surface is also described as a heart shape. The 3rd molar also shows greater developmental variation than either the 1st or 3rd molars, and are often the tooth that is congenitally missing. All roots of the molars angle distally with respect to the major crown axes (White & Folkens 2005: 152).
Mandibular Teeth:
Incisors
Lower incisor crowns are narrow compared to their height and have comparatively little lingual topography, further to this the roots are usually more mesiodistally compressed in cross-section (White & Folkens 2005: 139). The lower central incisor crowns are slightly smaller than the lower lateral crowns, with shorter roots relative to the crown and absolutely than lateral incisors (White & Folkens 2005: 142).
Canines
Lower canines have comparatively little lingual relief compared to the upper canines, and the apical occlusal wear is mostly labial. The lower canines are also narrow relative to their height (White & Folkens 2005: 139).
Premolars
Lower premolar crowns are more circular in occlusal outline than upper premolars, and have comparatively weak median line grooves. In lower premolars the long axes of the roots are angled distally relative to the vertical axis of the crown. When IPCFs are present they are mesial and distal in location (White & Folkens 2005: 150).
Molars
Generally speaking the mandibular molars go from largest (1st molar) to smallest (3rd molar) in size and morphology, same as the maxilla molars. The 1st mandibular molar is very recognizable as it has the largest crown with 5 cusps in the distinctive Y-5 cusp pattern and a pentagonal occlusal surface. The two roots of the tooth tend to be long, separate and divergent. The 3rd molar is smaller than the 1st or 2nd and have more irregular cusps and lack distal IPCFs, it also has two short and poorly developed roots that curve distally. The occlusal surface is often described as crenelated and ovoid in shape. The 2nd molar crown is an intermediate of the 1st and 3rd crowns (with 4 cusps) and roots (which have a distal inclination) in morphological terms, but has a distinctive +4 pattern of the occlusal surface. All roots of the molars angle distally with respect to the major crown axes.
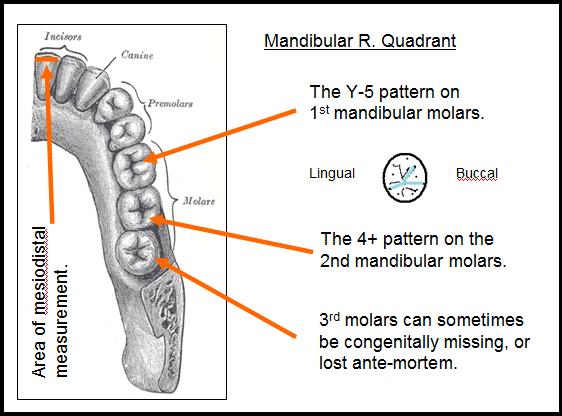
Graphic of the mandibular right quadrant highlighting a few of the specific dental anatomy terms from the above section. Image credit: modified from Gray’s Anatomy here.
Information for this section taken from White & Folkens 2005: 133-152 and here.
For tooth identification there are four questions to bear in mind:
A) To which category (or class) does the tooth belong?
B) Is the tooth permanent or deciduous?
C) Is the tooth an upper or a lower?
D) Where in the arch is the tooth located?
Although I’ve hinted at some of the answers above, those questions are a whole other post! But do investigate the Human Bone Manual by White and Folkens (2005) for further information and/or Brothwell (1981) and Mays (1999).
Note
This post will be updated to include the muscles of mastication.
Further Information
- Over at Bone Broke Jess Beck has a number of detailed posts focusing on teeth, with a few entries describing the anatomy of the various classes of teeth in detail (expect future posts though!). Particularly useful is the Identifying Human Teeth: Human Dentition Cheat Sheet post, which can handily be downloaded as a PDF.
- Check out this handy sheet for anatomical and direction terminology for teeth.
- The University of Illinois at Chicago have a wonderfully helpful molar identification sheet available here.
- Can teeth heal themselves? I wish! Only a bit by demineralization, learn more here.
- Over at What Missing Link? James R Lumbard has a fantastic post on how the muscles work, which includes a case study on the musculature of the jaw.
- An in-depth 13-minute dissection video of the muscles of mastication can be found here. Please be aware that this is a real human dissection.
Bibliography
Brickley, M. & McKinley, J. I. (eds.). 2004. Guidance to the Standards for Recording Human Skeletal Remains. BABAO & Reading: IFA Paper No. 7. (Open Access).
Brothwell, D. R. 1981. Digging Up Bones: The Excavation, Treatment and Study of Human Skeletal Remains. Ithica: Cornell University Press. (Open Access).
Connell, B. 2004. Compiling a Dental Inventory. In Brickley, M. & McKinley, J. I. (eds.) Guidance to the Standards for Recording Human Skeletal Remains. BABAO & Reading: IFA Paper No.7: 8. (Open Access).
Gosling, J. A., Harris, P. F., Humpherson, J. R., Whitmore I.,& Willan P. L. T. 2008. Human Anatomy Color Atlas and Text Book. Philadelphia: Mosby Elsevier.
Hawks, J. 2005. Caring for the Edentulous. John Hawks Weblog. Accessed 29th October 2014.
Koff, C. 2004. The Bone Woman: Among the Dead in Rwanda, Bosnia, Croatia and Kosovo. London: Atlantic Books.
Larsen, C. S. 1997. Bioarchaeology: Interpreting Behaviour from the Human Skeleton. Cambridge: Cambridge University Press.
Lewis, M. E. 2009. The Bioarchaeology of Children: Perspectives from Biological and Forensic Anthropology. Cambridge: Cambridge University Press.
Mays, S. 1999. The Archaeology of Human Bones. Glasgow: Bell & Bain Ltd.
White, T. & Folkens, P. 2005. The Human Bone Manual. London: Elsevier Academic Press.

.jpg%3Bhttp%253A%252F%252Fwww.thenextdds.com%252Fclinicalimages.aspx%253Fcatid%253D622%2526id%253D4294969603%2526y%253D2%2526t%253Di%3B495%3B375){kind=link}
{kind=link}
Reblogged this on Far off Places and commented:
Como antropóloga confesso que os dentes me dão grandes dor de cabeça! 🙂
This is great!
thanks! Need to update the mastication bits…
Very interesting and informative! I appreciate all the diagrams and images since it helps to have a visual example. Something I’ve always found curious was how children with congenital syphilis have notched teeth; I’d read about it all the time in medical history books, but never knew exactly what they meant until I saw some examples at the Hunterian Museum.
Cheers! Yeah, if I remember rightly they also have the mulberry molars (briefly mentioned in the post). I wished the post had a few more diagrams really and the space to go through each class of tooth properly, but space and google are limiting!
Reblogged this on AmiraZara.